|
Arrest of Active Labor |
|
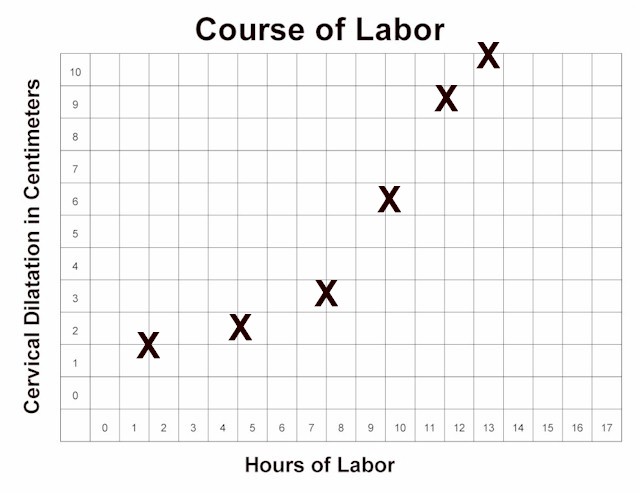
 Normal labor progresses slowly
during the latent phase. Then, after 4 cm dilatation, the more rapid,
active phase of labor begins. Normal labor progresses slowly
during the latent phase. Then, after 4 cm dilatation, the more rapid,
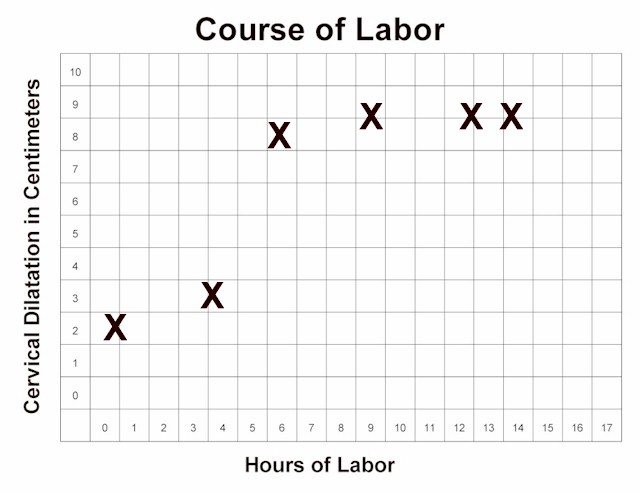
active phase of labor begins.During active labor (after 4 cm), the cervix should progressively dilate at a rate of no less than 1.2 cm/hour (for first babies) to 1.5 cm/hour (for subsequent babies). If active labor progresses more slowly than this, an "arrest of labor" has occurred. The arrest of labor may be simple slowing of the labor below the expected rate, or may represent a complete arrest, in which there is no further progress for at least 2 hours. There are essentially only two causes for an arrest of labor in the active phase:
Contractions may be inadequate because they are too infrequent (more than 4 minute intervals), or do not last long enough (less than 30 seconds). Typically, they are neither frequent enough nor long enough. Mechanical impediments to labor may include:
Inadequate contractions are treated with uterine stimulation. This is generally accomplished with intravenous oxytocin, delivered in steady, small amounts with a controlled infusion pump. The dose is started relatively low, and then advanced gradually until the desired effect is achieved. Later in labor, the dosage is often adjusted downward or stopped altogether if the contractions are too close together (consistently more than 5 contractions every 10 minutes). Amniotomy (artificial rupture of the bag of waters) can also be a
effective stimulus to labor. Amniotomy may be safely performed if the fetal
head is sufficiently engaged in the maternal pelvis to keep the umbilical cord
from slipping past it, creating a prolapsed cord situation. Nipple stimulation (rolling the nipple back and forth with thumb and forefinger) will cause of release of the mother's own oxytocin from her pituitary gland. This will have the effect of stimulating contractions. Stimulating both nipples will have about double the effect as stimulating one nipple. After about 15-20 minutes of nipple stimulation you will have released about as much natural oxytocin as is available. Nipple stimulation can be repeated at a later time, after the natural oxytocin supply has been replenished.
The possibility of a mechanical impediment should be considered whenever arrest disorders occur.
Usually, there is no way to know in advance which labors will experience an absolute obstruction and those that will not. For this reason, a trial of labor is almost always indicated. Those patients with an absolute obstruction will demonstrate a complete arrest pattern and will need cesarean section. |

{kind=link}
{kind=link}