|
Examining the Ears |

|
The ear is the primary organ of hearing. It is divided into three parts: the external, middle, and inner ear. External Ear The external, or outer, ear is composed of two parts, the auricle and the external auditory canal. The auricle, or pinna, is a cartilaginous structure located on each side of the head. The auricle collects sound waves from the environment, which are then conducted by the external auditory canal to the eardrum. The lining of the auditory canal contains glands that secrete a waxy substance called cerumen. The cerumen aids in protecting the eardrum against foreign bodies and microorganisms. The eardrum, or tympanic membrane, is an oval sheet of fibrous epithelial tissue, 10 mm by 9 mm in size, which stretches across the inner end of the external auditory canal and separates the outer and middle ear. The sound waves cause the eardrum to vibrate. This vibration transfers the sounds from the external environment to the auditory ossicles. Middle Ear The middle ear is a cavity in the temporal bone, lined with epithelium. It contains three auditory ossicles-the malleus (hammer), the incus (anvil), and the stapes (stirrup)-which transmit vibrations from the tympanic membrane to the fluid in the inner ear. The malleus is attached to the inner surface of the eardrum and connects with the incus, which in turn connects with the stapes. The base of the stapes is attached to the oval window (fenestra ovalis), the membrane-covered opening of the inner ear. These tiny bones link together to span the middle ear. They are suspended from its bony wall by ligaments and provide the mechanical means for transmission of sound vibrations to the inner ear. The eustachian tube connects the middle ear with the pharynx. It is lined with a mucous membrane and is about 36 mm long. Its function is to equalize internal and external air pressure. For example, while riding an elevator in a tall building, you may experience a feeling of pressure in the ear. This is usually relieved by swallowing, which opens the eustachian tube and allows the pressurized air to escape and equalize with the area of lower pressure. Divers who ascend too fast to allow pressure to adjust may experience rupture of their eardrums. The eustachian tube can also be a pathway for infection of the middle ear. Inner Ear The inner ear is filled with a fluid called endolymph. Sound vibrations that cause the stapes to move against the oval window create internal ripples that run through the endolymph. These pressurized ripples move to the cochlea, a small snail-shaped structure housing the organ of Corti, the hearing organ. The cells protruding from the organ of Corti are stimulated by the ripples to convert these mechanical vibrations into nerve impulses, which are relayed through the cochlear (8th cranial) nerve to the auditory area of the cortex in the temporal lobe of the brain. Here they are interpreted as the sounds we hear. Other structures of the inner ear are the three semicircular canals, situated perpendicular to each other. Movement of the endolymph within the canals, caused by general body movements, stimulates nerve endings, which report these changes in body position to the brain, which in turn uses the information to maintain equilibrium. The round window (fenestra rotunda) is another membranecovered opening of the inner ear. It contracts the middle ear and flexes to accommodate the inner ear ripples caused by the stapes. |
 Tragus Press
|
Examination of the Ear:
Hearing:
External ear (auricle or pinna)
Ear Canal
|
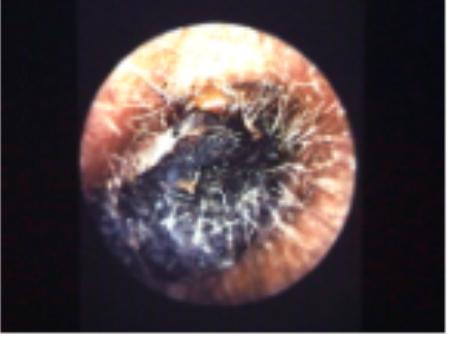 Cerumen Impaction |
Drum (Tympanic Membrane or TM)
|

Source: Operational Medicine 2001, Health Care in Military Settings, NAVMED P-5139, May 1, 2001, Bureau of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington, D.C., 20372-5300