|
Episiotomy |
 Sometimes, a small incision is made in the perineum to widen the vaginal
opening, reduce the risk of laceration, and speed the delivery.
Sometimes, a small incision is made in the perineum to widen the vaginal
opening, reduce the risk of laceration, and speed the delivery.
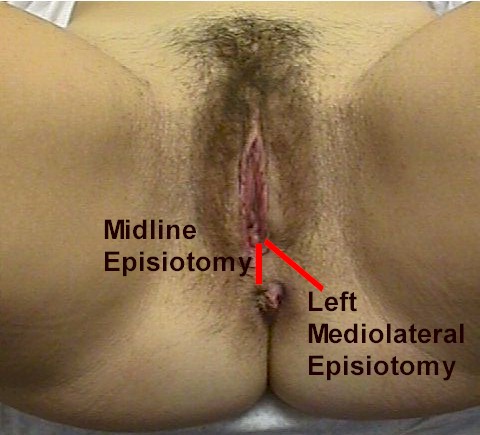
There are two forms, midline and mediolateral.
A midline episiotomy is safe, and avoids major blood vessels and nerves. It heals well and quickly and is reasonably comfortable after delivery.
If the fetal head is still too big to allow for delivery without tearing, the lacerations will likely extend along the line of the episiotomy. Lacerations through the rectal sphincter and into the rectum are relatively common with this type of episiotomy.
A mediolateral episiotomy avoids the problems of tearing into the rectum by directing the forces laterally. However, these episiotomies bleed more, take longer to heal, and are generally more uncomfortable after delivery.
If you don't perform an episiotomy, you are increasing the risk of vulvar lacerations, but these are usually (not always) small, non-threatening lacerations that will heal well without further complications. There may not be a laceration at all.
If you perform a midline episiotomy, you will have fewer vulvar lacerations, but the few you have are more likely to be the trickier 3rd and 4th degree lacerations involving the anal sphincter and rectum.
If you perform a mediolateral episiotomy, you will avoid the 3rd and 4th degree lacerations, but you may open the ischio-rectal fossa to contamination and infection and increase the intrapartum blood loss.
