|
Mild Dysplasia |
|
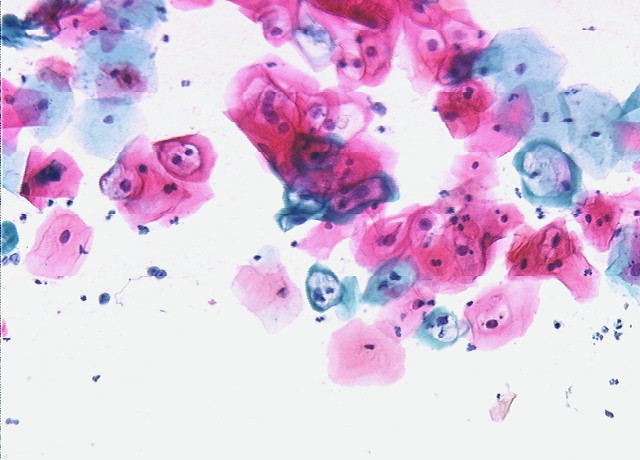
Mild dysplasia means the skin cells of the cervix are reproducing slightly more quickly than normal. The cells are slightly more plump than they should be and have larger, darker nuclei. This is not cancer, but does have some pre-malignant potential in some women. Other phrases that describe mild dysplasia include:
Many factors contribute the development of mild dysplasia, but infection with HPV, (Human Papilloma Virus) is probably the most important. Immune system impairment may also contribute. Mild dysplasia is not a permanent feature once it occurs. It can come and go, being present on a woman's cervix (and Pap smear) at one time and not another. This happens because the HPV virus that is a pre-requisite for these changes can lie dormant within the cervical skin cells. Normally held in check by the woman's immune system, the HPV can, at times of immune system distraction, reactivate the cellular machinery that leads to more rapid growth. For women who develop a single Pap smear showing mild dysplasia, there are basically three approaches that are commonly followed:
One common method of treatment of mild dysplasia is cryosurgery (freezing the part of the cervix containing the dysplastic cells and destroying those cells). Other approaches include vaporizing the dysplastic cells with a laser, or shaving them off with an electrified wire (LEEP). Sometimes, with very limited areas of dysplasia, the process of biopsy of that area removes enough tissue that the remaining dysplasia is sloughed off in the resulting eschar. In years past, we would often treat everyone with mild dysplasia vigorously to try to prevent progression to cancer. We had good results in about 90% of those treated. Unfortunately, all of the treatment modalities had about a 10% recurrence rate, not much different than if we had not treated them at all. If not treated, about 10% of women who develop mild dysplasia, will demonstrate a slow progression to moderate, then severe dysplasia, and ultimately develop invasive cancer of the cervix. This process generally takes about 10 years, although occasionally it can progress much more rapidly. The remaining 90% will either remain unchanged at mild dysplasia or regress back to normal. Currently, we usually just observe women with mild dysplasia with frequent Paps (every 3-6 months) over the next year or two, to discern those who will progress (the few) from those who remain unchanged or regress (the many). Those showing signs of advancement are then treated. This is based on the principles that:
There are plenty of exceptions to this general approach. Women whose access to medical care at a later time could be limited may benefit from more aggressive treatment. Those whose dysplasia covers an unusually wide area or whose lesion remains relatively inaccessible may also need to be treated. For women who have previously been evaluated with colposcopy and found to have dysplasia, the appearance of mild dysplasia on a subsequent Pap smear is not particularly alarming. Whether to re-colposcope them and the timing of such a re-evaluation must be individualized, based on the patient's history, risk factors, the degree of abnormality in the past and intervening Pap smear results. |