|
Breast Pain |
|
|
 Non-cyclic Breast Pain
Non-cyclic Breast Pain
Among the common causes of non-cyclic breast pain are trauma, infection,
and chest wall pain underlying the breast tissue (muscle strain or overuse of
the pectoralis major muscle). Breast cancer rarely causes breast pain in the
early stages and is not usually suspected unless the symptoms persist.
Hormonal causes include functional ovarian cysts and pregnancy.
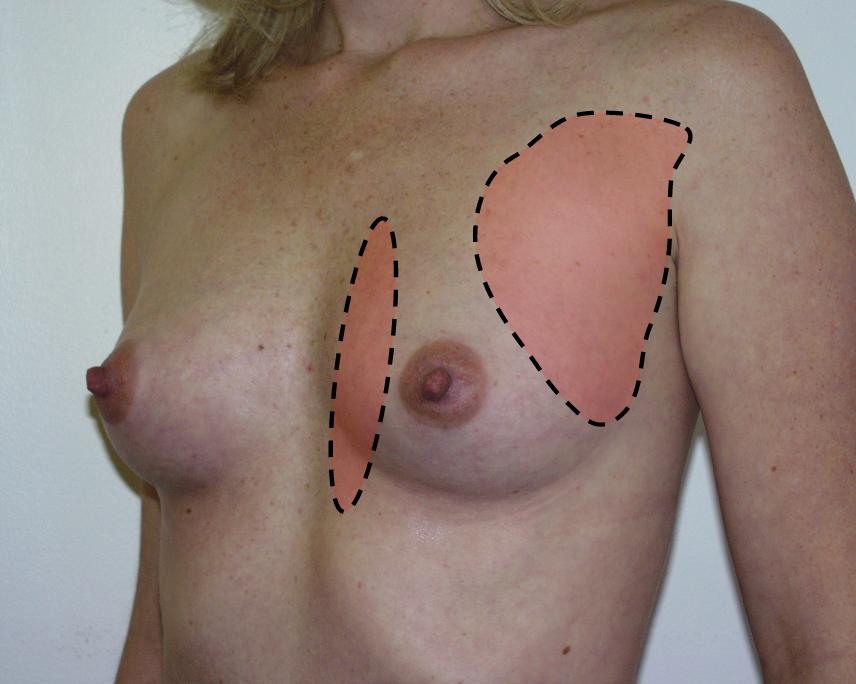
Women complaining of non-cyclic breast pain should have a careful examination. Common areas of tenderness include the pectoralis muscle distribution over the anterior chest wall. In this case, the muscle itself will be sore and the breast, if palpated with two hands and not pressed against the tender muscle, will be non-tender. Pain or soreness in the pectoralis major muscle is frequently found among women who have recently engaged in strenuous physical activity, and it represents a muscle strain. Chest wall pain does not involve the nipple or areola, while cyclic breast tenderness usually does. Treatment is symptomatic, with rest, some stretching exercises, and non-steroidal anti-inflammatory medication such as ibuprofen or naproxen.
A second common area for chest wall pain is along the costal margin. Direct pressure on the costochondral cartilage, without compressing breast tissue, will duplicate the pain. Compressing the chest wall with your hands placed laterally to the breasts will also duplicate the pain. This costochondritis has similar etiologies to the pectoralis major muscle tenderness, and the treatment is the same. and if the pain persists, referral will likely be necessary.
Trauma can include vigorous coughing or vomiting. The resulting strong, sustained contractions of the intercostal muscles can lead to chest wall tenderness that may be perceived by the patient as breast pain.
 Cyclic Breast Pain
Cyclic Breast Pain
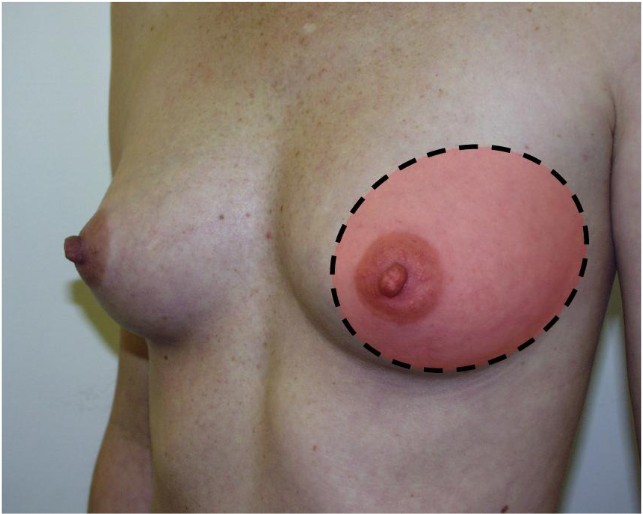
During the days leading up to the menstrual flow, the breasts normally are
somewhat engorged and may be somewhat tender. Following the onset of menstrual
flow, these changes spontaneously resolve. If the tenderness is more than mild
or is clinically bothersome, it is called cyclic breast pain or mastodynia.
If examined during this time, these women also often have significantly enhanced nodularity of the breast tissue. the combination of cyclic breast pain and symmetrically thickened nodularity of the breast tissue is often called fibrocystic disease (misnamed because it's not really a disease) or fibrocystic breast changes.
While not dangerous, women with cyclic mastodynia find it annoying and in its most severe form, interferes with some normal activities.
Some women find that by reducing or eliminating their intake of caffeine (coffee, tea, cola drinks) and taking Vitamin E supplements (400 IU daily) has seemed to improve their symptoms. Whether such improvement is pharmacologic or placebo in nature is still under debate.
Any pharmacologic approach that suppresses ovulation will be very helpful in treating cyclic mastodynia. Among these, birth control pills are the simplest. Taking BCPs in the usual fashion generally improves the pain significantly. For those who still experience significant pain, continuous birth control pills will usually suppress the pain completely.
Also effective, by virtue of ovulation inhibition, are depot medroxyprogesterone acetate, Lupron, or Danocrine, the latter two usually justified only in severe cases due to their significant side effects.