|
The Gynecologic Exam |

|
A gynecologic exam may be performed to evaluate a specific problem, or on a routine basis as screening for healthy lifestyles and subclinical disease. Routine exams are usually performed annually among women of childbearing years. The amount of detail and the content of the exam will depend on many factors, but may include: For a new patient, your history-taking and physical examination will take longer than for a patient you've seen before and know well. For returning gynecologic patients, your history and physical will likely be more focused. |
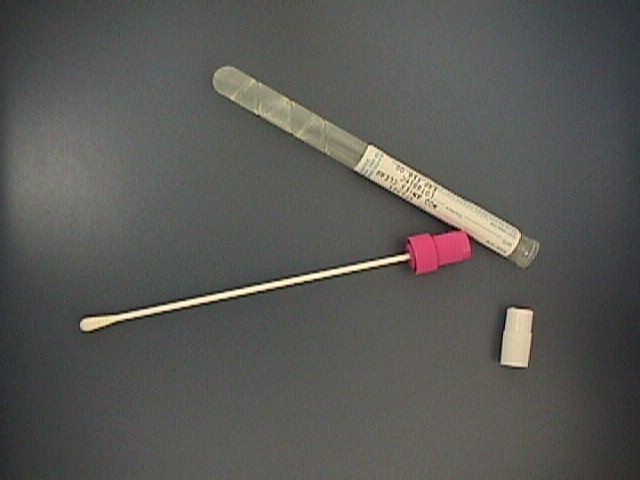 |
Cultures Bacterial cultures for Strep, E. coli and other pathogens may then indicate a course of treatment that would not necessarily be obvious from either the gross appearance of the vagina or the wet mount. Some physicians routinely culture for gonorrhea and/or chlamydia on all of their patients at each routine visit. Others culture for these STDs only among high risk patients or those with unexplained pelvic pain. The wisest course for you depends on the frequency with which these STDs are found in your population. |
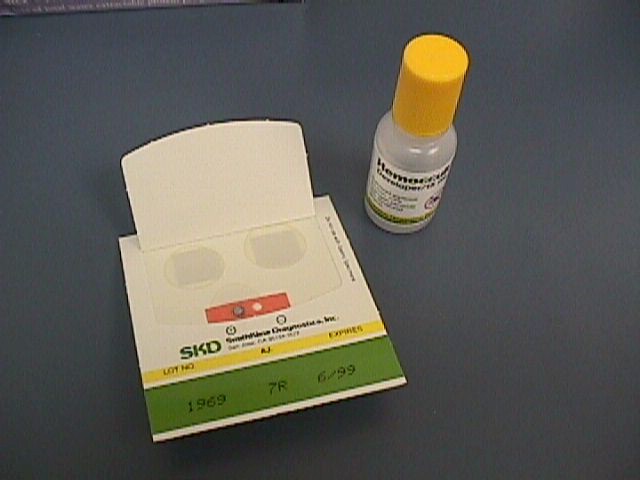 |
Rectal Routine screening with sigmoidoscopy every 5 years after age 50 is recommended by many physicians. After the rectal exam, the small particles of stool left on the examining glove can be evaluated for the presence of occult blood. This is most useful after the age of 50. |
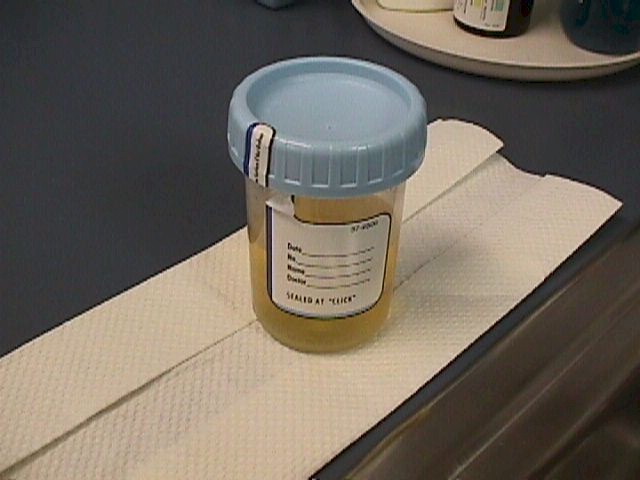 |
Urine Others check the urine only for a specific indications. A clean urine specimen can be evaluated for the presence of:
|
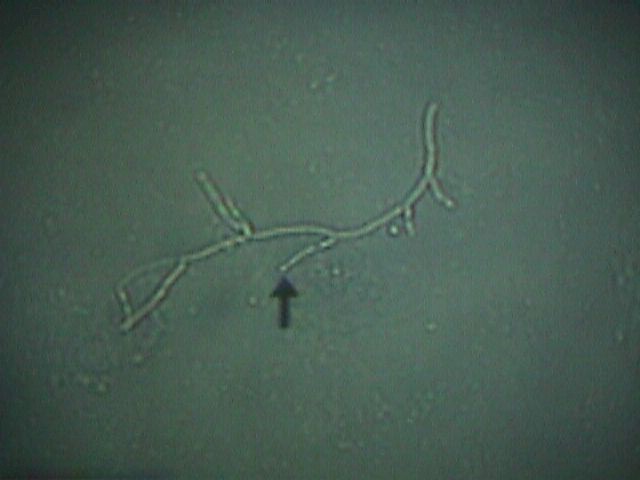 Yeast on high power |
Wet Mount Mix a small amount of discharge with 10% potassium hydroxide (KOH), place it on a glass slide and cover it with a coverslip. The KOH dissolves cell membranes, making it easier to see yeast organisms under the microscope. Mix another small amount of discharge with a drop of normal saline, place it on a glass slide with a coverslip, and examine it under the microscope. With saline, active trichomonad organisms can be seen moving and "clue cells," indicating bacterial vaginosis can be seen. |
 |
Mammography While not 100% accurate, mammography is probably around 80% accurate, particularly in detecting the very small, early malignancies not appreciated by physical examination. Recommendations for frequency of mammograms vary, but the following general guidelines can be followed:
|
 |
Breast Self-examination
Many offices use a video to demonstrate breast examination techniques. Some use a manikin with several breast lumps for the patient to identify. Some have a patient information sheet the woman can take home to study on her own. |
 |
Counseling It may be focused on the problems presented during the examination, or may be global, such as diet, exercise, or other healthy life-styles. Patients often feel this is the most important part of the visit. Take your time and sit down while talking to the patient. You need not be a master of "bed side manner" for the patient to appreciate this time. Just be honest, direct, and pleasant. Plan Laboratory requisitions or consultation requests can be given. Patient hand-outs can be provided. Plans might include:
It is routine to indicate when the patient should return to the office (RTO) or return to the clinic (RTC).
|
 |
Charting
|
