|
Menopause |
Many people view menopause as a distinct point in time, beyond which all ovarian function ceases. That might be true for a few women, but for most, menopause is a more gradual process, characterized by waxing and waning ovarian function over a period of many years. During this time, ovarian function may cease altogether for a few months (accompanied by vasomotor symptoms and amenorrhea), only to return (with disappearance of the symptoms and resumption of menstrual flows). This "off again, on again" pattern is not at all unusual and is probably more the rule than the exception. This many-year period of time is frequently called "peri-menopause." Physiology
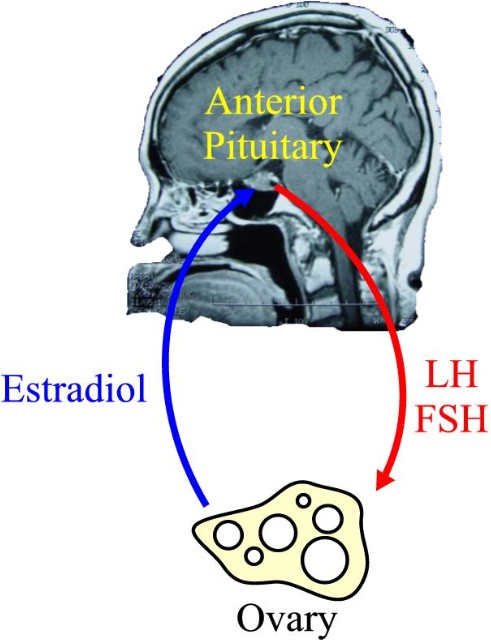
During the reproductive years, the ovaries function under control of the anterior pituitary gland, through its release of follicle stimulating hormone (FSH) and luteinizing hormone (LH). This causes production of estrogen (quite a bit), progesterone (some), testosterone (not much, but very important), and ovulation. Of these functions, ovulation is the most complex, while production of testosterone is the simplest. The estradiol (estrogen) produced by the ovary circulates through the woman's bloodstream to receptors in the brain (primarily anterior pituitary), where it inhibits release of FSH. Consequently, the stimulus to the ovary to produce its hormones and release its eggs diminishes, menstruation occurs, and the whole process begins anew. Menopause occurs because the ovaries stop responding to FSH and LH, not because the brain stops releasing FSH and LH. A menopausal woman will generally have very high levels of FSH and LH, but very low levels of estrogen (estradiol) in her bloodstream.
Symptoms
Women slowly lose bone mass, starting at a relatively early age. Menopause rapidly accelerates this process, resulting in osteopenia (decreased bone density) or osteoporosis (so much bone loss that pathologic fractures are a realistic possibility). The incidence of heart disease also increases rapidly after menopause. During their reproductive years, women enjoy a substantial advantage over men in heart disease. With menopause, the risk of heart disease among women rises to that of men, with women losing the relative protection that they had earlier.
Osteoporosis Taking extra calcium (1000-1500 grams of elemental calcium/day) is helpful in preventing osteoporosis, but the help is very small. Similarly, regular weight-bearing exercise is helpful, but only to a limited extent. Taking estrogen helps a great deal, but usually won't reverse the effects of osteoporosis. Bisphosphonates, such as alendronate are even more powerful and can reverse osteoporosis, although they can cause significant side effects. Increased risk factors for osteoporosis include:
Bone density studies (Dexa Scan) will show a T-value of -2.5 or worse among women with osteoporosis. Osteopenic women have T-values of -1.0 to -2.5.
One philosophy holds that:
The other philosophy holds that:
Given these two differing philosophies, it is not difficult to imagine that there are disagreements among conscientious practitioners as to the proper role of estrogen replacement therapy. Menopause is a relatively new issue in the human experience. Until recently, very few women lived long enough to reach menopause. The average life expectancy for women in North America in 1900 was age 42. Currently it is age 82. Because of this, our clinical experience with large numbers of menopausal patients is really limited to the last century. As physicians, I expect we will learn a great deal more about menopause in the coming century, when the philosophical differences may be resolved.
It is also probably true that estrogen replacement therapy:
Taken alone, estrogen replacement in standard doses is associated with an increased risk of uterine cancer. The addition of progesterone to the estrogen not only blocks the increased risk of uterine cancer, it reduces the risk to less than that of women who don't take any ERT at all. For this reason, progesterone has routinely been added to estrogen replacement regimens for women who have uteruses. Women who have undergone hysterectomy have no need for the progesterone addition. Progesterone blunts, to some extent, some of the other estrogenic effects, and the best of the long term studies have not reported their results from estrogen-alone therapies. It is possible that some of the risks of ERT are actually a result of the progesterone.
For many women, this 30% drop in testosterone will be unnoticed. For others, they may experience symptoms of low testosterone, the most prominent of which are lethargy and decreased sex drive. For women with complaints of lethargy and decreased libido during menopause, some physicians will routinely measure serum testosterone. If testosterone levels are relatively low, these women may benefit from a therapeutic trial of small doses of testosterone, usually in addition to estrogen replacement. Serum testosterone levels are followed to make sure that the woman is not receiving too much hormone. Many women find this combination neatly resolves their symptoms. Not everyone benefits from this regimen. Some have side-effects (hair growth, voice changes, adverse lipid changes), that require stopping the testosterone. Others notice no difference in their energy levels or libido.
A number of satisfactory treatment strategies and doses are available for estrogen replacement therapy. They include both continuous and cyclic approaches. The benefits to continuous therapy are simplicity and absence of menstrual bleeding in the majority of women. For a minority, spotting or breakthrough bleeding complicate continuous therapy and these women generally do better on a cyclic approach. For those on cyclic therapy, 1/3 experience normal menstrual flows, 1/3 have no periods at all, and 1/3 will initially experience menstrual flows, but the flows will gradually abate over time. The following are examples of typical ERT doses: Once the patient is started on the estrogen replacement, it is important to see how she's doing in 1-3 months after starting it. If she continues to have vasomotor symptoms, then she needs a higher dose of estrogen. If she has persistent breast tenderness or headaches, she may be getting too much estrogen. Measuring serum estrogen (estradiol) levels may prove helpful in managing such women.
Blood estrogen levels may be useful in the management of many menopausal women and their estrogen replacement therapy. During the reproductive years, estrogen levels vary with the menstrual cycle: In menopause, the estradiol levels typically are less than 32 pg/ml and often <10. When treating menopausal women with estrogen, a reasonable target would be estradiol levels of 50-100 pg/ml. If the patient has levels a little higher or lower, but feels fine, then she can remain on the same dose. However, a woman on standard doses of estrogen who continues to have vasomotor symptoms and whose estradiol level is only 40 will likely benefit from a higher dose, nudging her into the typical therapeutic range.
It is relatively common for women who are started on estrogen replacement therapy to resume some degree of ovarian function. Giving estrogen will inhibit the release of FSH and LH and serum levels of these gonadotropins will fall. Then, in response to stopping the estrogen (as in some forms of cyclic therapy), the FSH will again rise. The ovaries, particularly if they are still relatively close to the time of menopause may respond briefly to the rising level of FSH, even though they didn't respond to the sustained high levels of FSH. Such an occurrence can lead to brief resumption of estrogen production (and resultant estrogen excess symptoms of breast tenderness or bleeding), or even ovulation (resulting in a full-blown menstrual period two weeks later). Pregnancy occurring in this circumstance would be very unlikely because the the quality of the older ovarian follicle is usually poor. The main problem is an unexpected menstrual flow occurring in a woman who was advised she was menopausal and who is now receiving treatment for menopause. An advance explanation of this possibility will relieve the patient's anxiety and concern over the depth of your knowledge and skill. At least two approaches to this problem can be effective:
|
||||||||||||||||||